|
Purpose |
In high volume, critical, practices and emergency department-based practices, especially in level 1 trauma centers, there are often several studies on the worklist that may be deemed acute and in need of prompt radiological attention. As the number of algorithms to evaluate various acute pathologies increases, an understanding of the prioritization of acute and non-acute relay of findings needs to be developed in worklist prioritization algorithms. Algorithms need to intelligently prioritize studies based on the acuity of findings, patient condition, and turn-around time standards. |
|
Tag(s) |
Non-Interpretative ,worklist Management worklist prioritization |
|
Panel |
Reading Room |
|
Define-AI ID |
19120004 |
|
Originator |
Melissa Davis |
| Lead | Melissa Davis |
|
Panel Chair |
Ben Wandtke |
| Non-Interpretative Panel Chairs: | Alexander J Towbin, Adam Prater |
|
Panel Reviewer |
Reading Room Subpanel |
|
License |
Creative Commons 4.0 |
| Status | Public Commenting |
Clinical Implementation
Value Proposition
Prioritizing imaging studies is an important part of day to day workflows within the radiology reading room. Historically, cases have been flagged by the ordering provider with an advanced order priority (i.e. STAT), by the ordering provider by indicating order type (i.e. MRI for Stroke), by the time of the order or completion of the imaging study (i.e. first-in, first out); by the location of the patient (i.e. the emergency room), by the technologist performing the study or resident reviewing the study as needing to be looked at sooner rather than later. With new acute finding detection algorithms, there is a need to understand levels of acuity within positive findings cases, as well as keep workflow moving for non-acute finding cases. The goal of this use case is to create an algorithm that prioritizes the worklist while taking into account patient setting, acuity of findings, and turn-around time expectations. The machine learning tool could learn from past radiologist workflows and practice standards/preferences to better prioritize cases on the worklist
Narrative(s)
In a level 1 trauma center the emergency department is often faced with a multitude of patients demonstrating varying levels of clinical concern. Several algorithms have been placed on their platform to identify acute pathology on imaging and alert the interpreting radiologist, including a platform to look for head bleeds, pulmonary emboli, and cervical spine fractures (ID# 18050006). The group anticipates that algorithms for the detection of additional pathologies such as pneumothorax (ID# 18080001), long bone fractures (ID# 18050009, 18050010, 18050018), and dissections may soon be available. When several studies are on the worklist with acute pathologies, understanding which studies are the most life threatening and need to be looked at first is important. This work is currently done through receiving alerts from the technologists or residents of a life-threatening finding, reading based on time the study was completed, or by glancing through a series of studies and making a determination on what should be read next. Additionally, in the emergency department, quality of care is often determined by time-based metrics. For patients with normal exam, having a quick disposition leads to greater patient satisfaction and ER physician satisfaction. These studies are often very quick reads compared to positive studies and help with vital triage functions so patients can flow in and out of the emergency department. Under the current circumstances, the radiologist may spend hours interpreting positive cases and neglect negative cases with a real impact on the patient care pathway. The ideal algorithm would prioritize studies by the acuity of pathology and understand turnaround time practice standards to not deprioritize non-acute, but disposition dependent and clinically relevant, examinations. The algorithm can insert appropriately these non-acute studies into the queue.
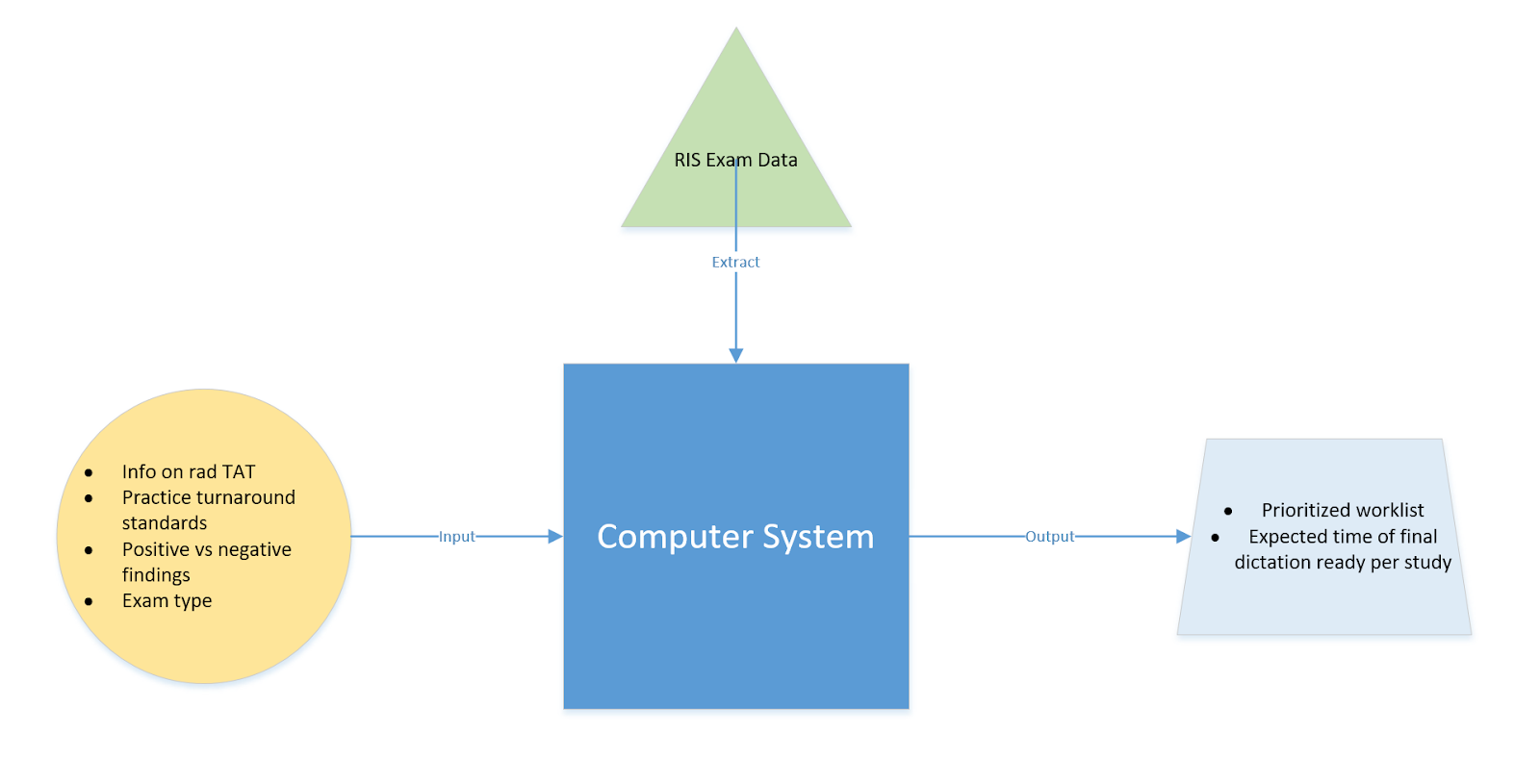
Workflow Description
The algorithm is autoloaded into the user's worklist for prioritization. The algorithm takes into account study status, acuity of findings from image interpretation algorithms, turn-around time practice standards (which may vary depending on the patient's location), study type, and study protocol. This means that the algorithm will take into account the acuity of findings throughout the worklist, and not deprioritize similarly acute findings. The algorithm will also take into account clinical information from the electronic health record, including laboratory values, vital signs, and clinical history, to aid in prioritization. This may mean that patients acutely ill and in need of immediate triage, but who may not have classically acute findings on imaging, are not deprioritized. The algorithm will also learn the dictation speed of each radiologist based on findings (normal and abnormal) and study type. Studies will be ordered in the user’s worklist to optimize relay of acute findings and triage capacity of the ordering providers.
Technical Specifications
Inputs
Exam Characteristics
|
Definition |
Features of an exam such as modality, location of exam, acute findings detected, body part, exam status (i.e., stat, routine, urgent, life-threatening), patient demographics, referring provider, and indication |
|
Potential Features
|
Modality, body part, patient demographics (age &sex), indication, referring provider, exam status, detection of an abnormality, location of exam(point of service in location in hospital), order priority, exam protocal |
Individual Radiologist Information
|
Definition
|
Information on each radiologist in the practice based on the selection criteria of the facility. This may include radiologist’s rate of dictation and subspecialty expertise and if working with a trainee. In the case of trainee assisted dictation, the resident or fellow rate of dictation could be accounted for based on prior experience, or a standard rate for trainee assisted work could be set. |
|
Potential Features
|
Radiologist turn-around time (based on study type and positive vs negative) , Radiologist Expertise
|
Radiologist Turnaround Times
|
Definition
|
Delivery of timely information to the healthcare team as needed; can be defined as the time from report available on the worklist for interpretation to the final report signed |
|
Potential Features |
Turnaround time, based on study type and positive vs. negative study |
Ordering Provider Characteristics
|
Definition |
Information about the Ordering Provider and their attributes that might affect the study delivery |
|
Potential Features
|
Ordering Provider Name, Speciality of Ordering Provider, Specified preferences from ordering providers on a specialty or subspecialty to read the study |
Primary Outputs
Optimal Worklist Priority
|
RadElement ID |
N/A |
|
Definition |
Fully optimized worklist to relay acute findings and triage patients in a timely manner |
|
Data Type |
N/A |
|
Value Set |
N/A |
|
Units |
N/A |
Secondary Outputs
Time to Next Study
|
RadElement ID |
N/A |
|
Definition |
Indicator for when a study will be completed based on historical inputs from the radiologist |
|
Data Type |
N/A |
|
Value Set |
N/A |
|
Units |
N/A |
Figures
References
-
Halsted MJ, Froehle CM. Design, implementation, and assessment of a radiology workflow management system. AJR Am J Roentgenol. 2008 Aug;191(2):321-7. doi: 10.2214/AJR.07.3122.
-
Gaskin CM, Patrie JT, Hanshew MD, Boatman DM, McWey RP.. Impact of a Reading Priority Scoring System on the Prioritization of Examination Interpretations.AJR Am J Roentgenol. 2016 May;206(5):1031-9. doi: 10.2214/AJR.15.14837.