|
Purpose |
To develop a system that facilitates the use of the lexicon and follow-up guidelines for incidental thyroid nodules, to drive consistency in radiology reporting and adherence to national guidelines. |
|
Tag(s) |
Non-Interpretative, Structured Reporting, Population Health Structured Recommendations, TIRADS |
|
Panel |
Population Health |
|
Define-AI ID |
19130001 |
|
Originator |
Shlomit Stein, Marta Heilbrun, Nina Kottler |
| Lead | Shlomit Stein, Marta Heilbrun, Nina Kottler |
|
Panel Chair |
Nina Kottler |
| Non-Interpretative Panel Chairs: | Alexander J Towbin, Adam Prater |
|
Panel Reviewers |
Population Health Subpanel |
|
License |
Creative Commons 4.0 |
| Status | Public Commenting |
Clinical Implementation
Value Proposition
The goal of the radiology report is to provide timely, actionable and accurate information to referring providers, the healthcare team, patients and their families. However, there is wide variability in radiology reporting language, content, structure, and recommendations across practices, which leads to increased cost, poor patient outcomes, and malalignment with national standards. Therein lies the need for consistent reporting. This use case can be used to improve accuracy and risk stratification for our patients. Reporting that is tied to a standardized lexicon and is subsequently validated clinically and pathologically, may also serve as the annotations for future work in pixel based analytics.
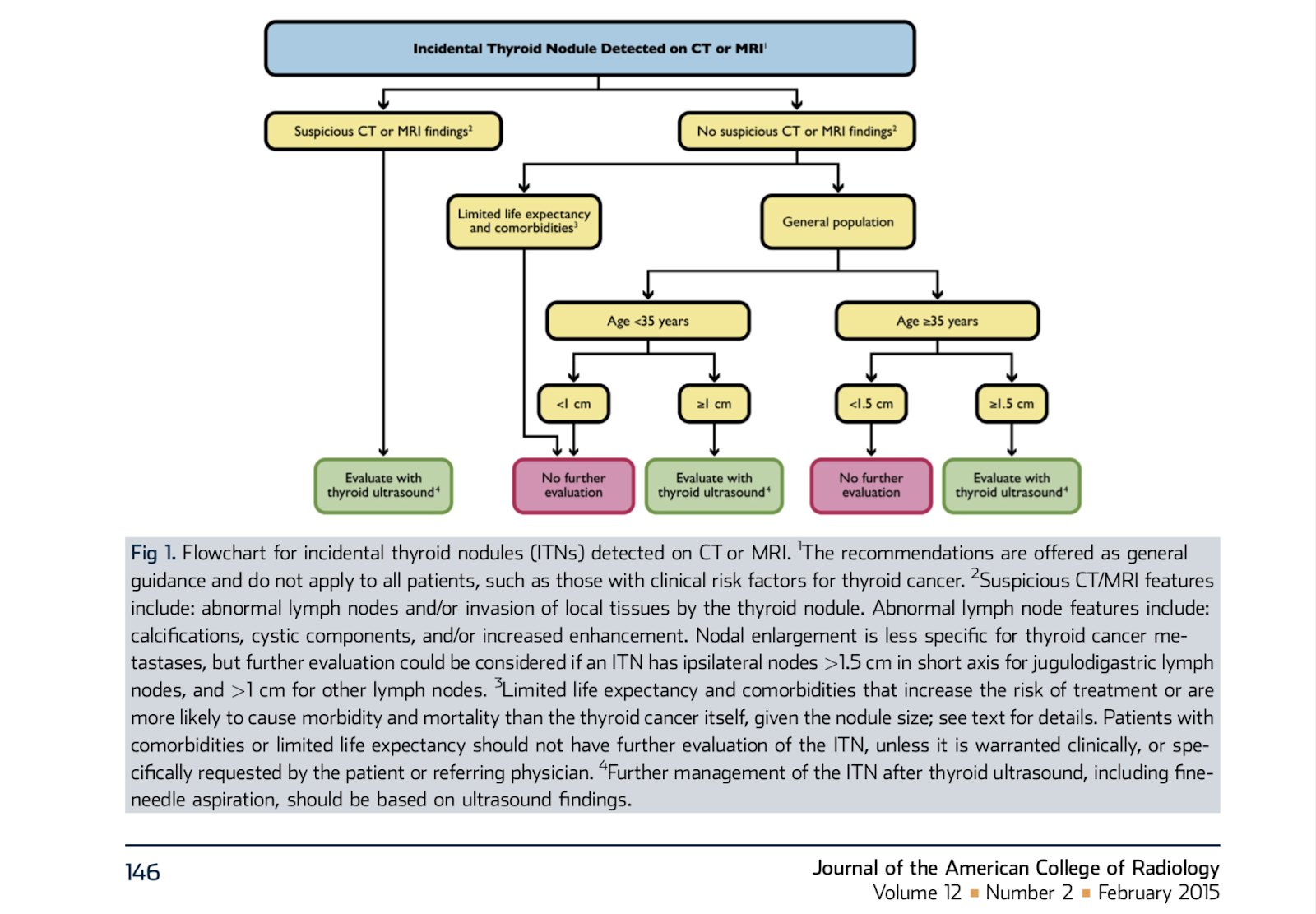
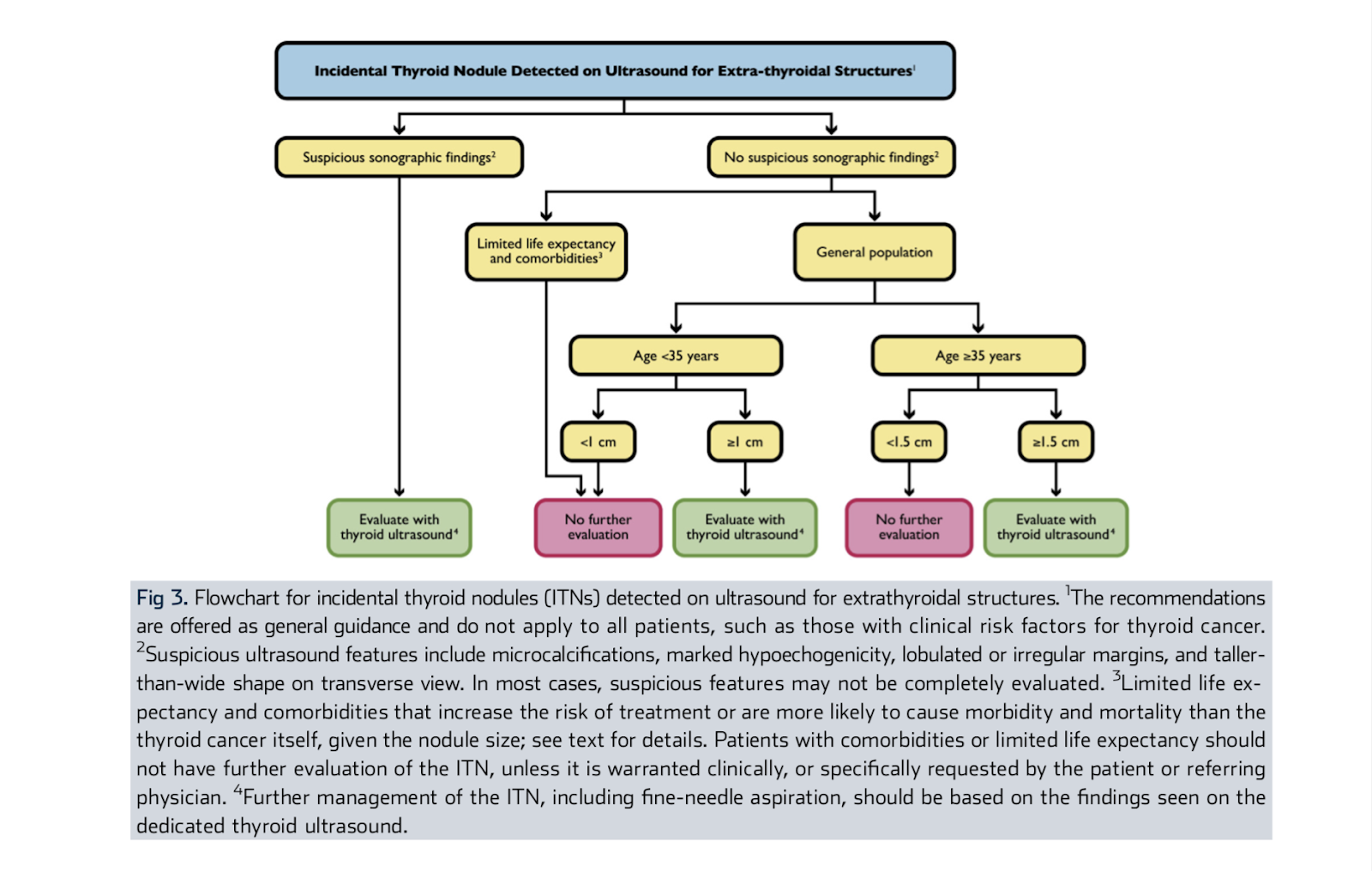
Thyroid nodules are some of the most commonly detected observations on cross-sectional imaging of the neck. The vast majority are benign, or if malignant, indolent in behavior. Those nodules that were not previously known or the characterization of such were not the indications for the examination are defined as incidental thyroid nodules (ITN). The ACR convened the Incidental Thyroid Findings Committee in 2013, with the goal of developing evidence and consensus based recommendations for the radiologist to use when ITNs are encountered. Figures from the Consensus White paper are attached. For CT and MR it is a 3-tier system of categorization, using imaging features, patient age, and size of the nodule. For FDG-PET and other nuclear medicine studies, recommendation depends on metabolic activity. For US it is a 3-tier system of categorization, using imaging features, patient age, and size of the nodule. Consistent use of these recommendations could reduce the burden of additional evaluation and workup with a very low likelihood of missing a clinically significant malignancy.
Narrative(s)
A patient comes in for a CT or MRI and the radiologist identifies an incidental thyroid nodule. The radiologist is expected to describe the nodule and provide the appropriate recommendations for further evaluation or workup of the observation.
Workflow Description
Optimally, the algorithm (1) identifies when a population health recommendation is applicable based on the reported information of a thyroid nodule (within the Findings and/or Impression segments of the radiology report) and (2) prompts the radiologist with the appropriate follow-up guideline based on identified inputs (modality, patient age, life expectancy/comorbidities, and reported findings including nodule size). The provided data should be automated where applicable, and were not, easy to input into the radiology report (single click or voice command), contain the reference used for the recommendation, and easy for the radiologist to validate. The radiologist could agree or disagree with the provided recommendation. If the radiologist agrees, the finding, recommendation, and reference should be placed in the Impression section of the radiologist report. If the radiologist disagrees, this feedback should be used to improve the tool for a subsequent release.
If both the Findings and Impression sections of the radiologist report are utilized, the algorithm will need to correlate the thyroid pathology between these two sections. If there are multiple findings in the thyroid gland, the algorithm should be able to determine which meets criteria for the most “severe” recommendation (ie thyroid ultrasound evaluation required), and provide follow-up based on that nodule or nodules. Finally, if more than one dimension is reported for a thyroid nodule, the largest dimension should be utilized for follow-up determination.
To accomplish these requirements, an interactive User Interface should be created for placement on the radiologist’s workstation. The user interface should display the extracted thyroid pathology name and size, the recommended follow-up, an option to agree and disagree with the provided recommendation, and a selection to insert the recommendation (and reference) into the report.
Considerations for Dataset Development
What procedures might prompt this algorithm?
CT Chest, C-spine, Neck; CTA Chest, Neck; MRI c-spine; MRA neck; MRI neck; US Neck (not specifically being performed for thyroid nodule evaluation).
CT: Computed Tomography
CTA: Computed Tomography Angiography
MR: Magnetic Resonance
MRA: Magnetic Resonance Angiography
US: Ultrasound
What do you consider an incidental thyroid nodule?
As defined within: Managing Incidental Thyroid Nodules Detected on Imaging: White Paper of the ACR Incidental Thyroid Findings Committee: J Am Coll Radiol 2015;12:143-150. It is defined as a nodule identified by an imaging study that was not previously detected or suspected clinically.
Technical Specifications
Inputs
ACR White Paper (REF 1)
|
Definition |
Follow-up guidelines for incidental thyroid nodules based on the ACR consensus white paper (REF 1) |
|
Potential Features |
Body part, incidental, non-incidental, thyroid nodule, lymph node |
Exam and Patient Metadata
|
Definition |
Features of an exam such as modality, body part, patient demographics (age), referring provider, all of which could be extracted from the RIS |
|
Potential Features |
Modality, Body Part, Patient Demographics (age) |
The Radiologist’s Report
|
Definition |
Information dictated by the reading radiologist. Each section of the report should be utilized including Exam, History, Comparison, Technique, Findings, and Impression. |
|
Potential Features |
Exam, history, technique, findings, impression |
Primary Outputs
Recommendation for Follow-Up
|
Definition |
Follow-up Ultrasound (US) or “No follow-up” recommendation(s) based on the ACR White Paper (REF 1). |
|
Data Type |
Text |
|
Value Set |
“No follow-up imaging recommended” or “Recommend ultrasound follow-up” |
|
Units |
N/A |
ACR White Paper Reference
|
Definition |
Appropriately referenced journal article or other peer reviewed literature from which the recommendation was based |
|
Data Type |
Text |
|
Value Set |
Managing Incidental Thyroid Nodules Detected on Imaging: White Paper of the ACR Incidental Thyroid Findings Committee. Hoang, Jenny K. et al. Journal of the American College of Radiology, Volume 12, Issue 2, 143 - 150. |
|
Units |
N/A |
Pathology Name that Triggered the Recommendation
|
Definition |
The pathology (e.g., thyroid nodule) extracted from the radiologist’s report |
|
Data Type |
Text |
|
Value Set |
thyroid nodule, thyroid mass, thyroid lesion, and other synonyms |
|
Units |
N/A |
Pathology Size that Triggered the Recommendation
|
Definition |
The size of the pathology (e.g., 3.2 cm) extracted from the radiologist’s report. |
|
Data Type |
Numeric |
|
Value Set |
number with one possible decimal point |
|
Units |
cm |
Reason why a recommendation is not provided for a thyroid nodule
|
Definition |
The ACR White Paper (REF 1) is applicable only for incidental thyroid nodules. If there is a suggestion that a thyroid nodule is not incidental, the algorithm should not produce a follow-up recommendation but rather output the non-incidental nature of the thyroid lesion in the user interface. |
|
Data Type |
Text |
|
Value Set |
“Non-incidental thyroid nodule identified; thyroid best practice does not apply” |
|
Units |
N/A |
Secondary Outputs
Confidence of recommendation- tool to correlate confidence with disagrees
|
Definition |
An assessment of the recommendation accuracy |
|
Data Type |
Numeric |
|
Value Set |
0-100 |
|
Units |
N/A |
Location of Lesion within the Thyroid Gland
|
Definition |
location of the pathology within the thyroid gland (the laterality is used in those reports that describe lymphadenopathy because laterality is required to determine if the lymph nodes are suspicious) - use standard language (CDE) |
|
Data Type |
Text |
|
Value Set |
right, left, bilateral, isthmus |
|
Units |
N/A |
Suspicious Features
|
Definition |
absence or presence of suspicious features including abnormal regional ipsilateral lymph nodes and invasion - use standard language (CDE) |
|
Data Type |
Text |
|
Value Set |
suspicious CT/MRI lymph node features (calcifications, cystic components, and/or increased enhancement; lymphadenopathy is less specific for thyroid cancer metastases but further evaluation can be considered for ipsilateral lymph nodes meeting the following size criteria jugulodigastric lymph node >1.5 cm in short axis, and other lymph nodes >1 cm in short axis ) and/or invasion of the thyroid lesion into the adjacent soft tissues |
|
Units |
N/A |
Figures

References
1. Managing Incidental Thyroid Nodules Detected on Imaging: White Paper of the ACR Incidental Thyroid Findings Committee. Hoang, Jenny K. et al. Journal of the American College of Radiology, Volume 12, Issue 2, 143 - 150.